Mental Health/Drug and Alcohol SAER Review Sub-Committee
The Mental Health/Drug and Alcohol SAER sub-committee review reports that involve patients/consumers receiving care from mental health and drug/alcohol services. This sub-committee reviewed 83 SAERs during the reporting period. The majority of SAERs were confirmed as a Harm Score 1 (93 per cent, n=77), followed by Harm Score 2 (5 per cent, n=4) and Harm Score 4 (2 per cent, n=2).
Review of Mental Health/Drug and Alcohol SAERs the following top human factor elements:
- No human factors identified, following review of the SAER report
- Loss of situation awareness, which relates to the fixation on irrelevant information, poor prioritisation and planning of care
- Skill-based – poor task execution, relating to failures in carrying out actions of a task, where the process was correct, but the execution was not.
- Cognitive based errors, involving the failure to understand, process or act appropriately on available information despite adequate education and knowledge.
- Knowledge based errors, that are caused by gaps in staff skills or knowledge
The top 5 clinical risk factors that were considered a direct cause, or contributing factor, to the outcome of an incident related to:
- Risk assessment – MH, relating to the accuracy, completion, and timeliness of mental health risk assessments
- Comorbidities – Physical, refers to the presence of two or more overlapping conditions in the same person
- Deteriorating patient – failure to recognise, patient deterioration was not recognised
- Drug and alcohol assessment, problems relating to the assessment of drug and alcohol issues
- Drug and alcohol referral, where the referral to drug and alcohol services was an issue
An overview of Mental Health/Drug and Alcohol SAER classifications are provided below.
Figure 11.
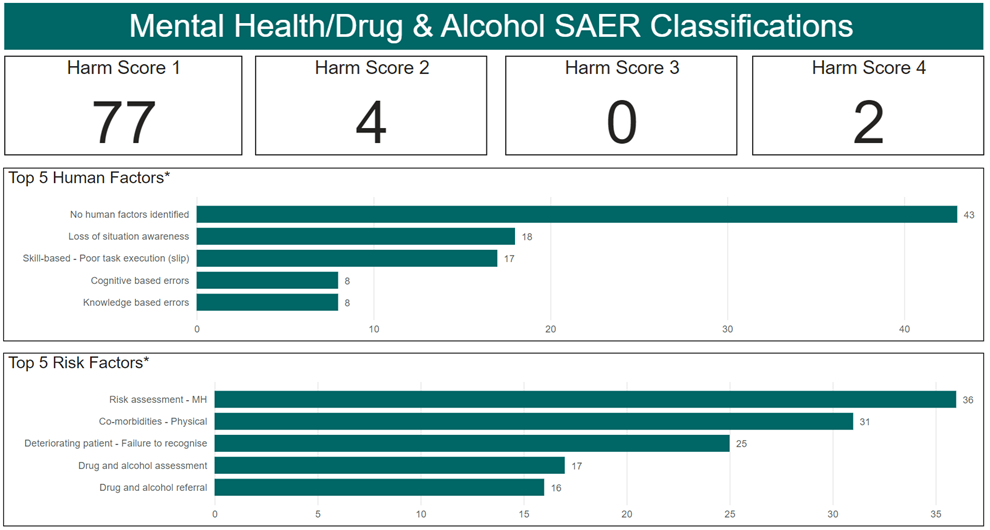
*Multiple factors can be applied to each SAER
System factors identified within the Mental Health/Drug and Alcohol SAER reports predominately related to:
- Care Planning, is further categorised into sub-categories related to care coordination, care plan development, the role of the patient, family and carers in care planning, risk assessment and communication deficiencies when implementing the care plan.
- Communication, is further categorised into sub-categories related to documentation, communication among clinicians and with the patient, family or carer.
- Assessment, is further categorised into sub-categories related to risk assessment, assessment of the patient's physical and mental health and assessment of concerns raised by patients, family and carers.
Figure 12.
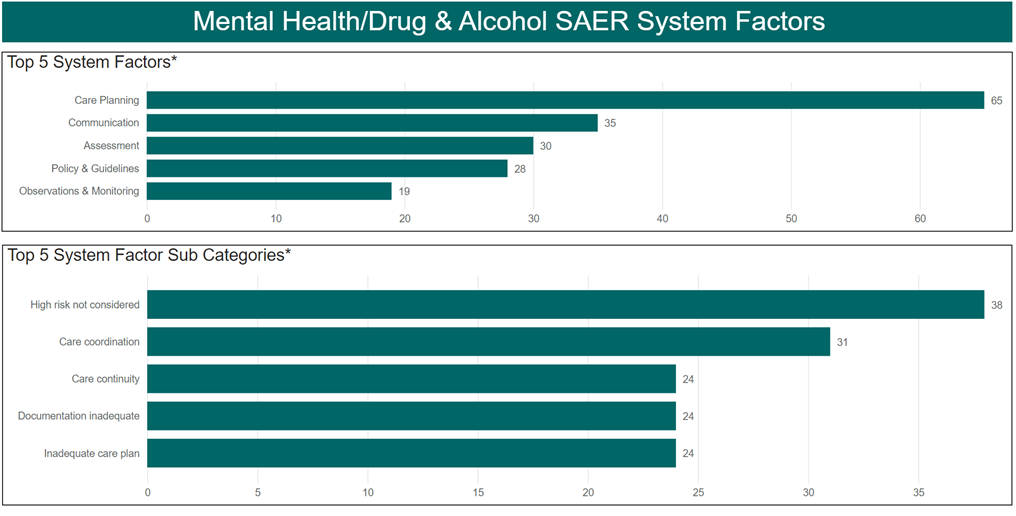
*Multiple factors can be applied to each SAER